

It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Some trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics” has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
The Myths (Part 1) …
Myth 1: 98% of all studies in this area were ignored
Myth 2: Cass recommended no Trans Healthcare for Under 25s.
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.
The Myths (Part 2)…
Myth 5: The Cass Review is worthless because it is not Peer Reviewed
Myth 6: The proposed service is based on the idea that brains don’t reach maturity until 25.
Myth 7: Most other systematic reviews and clinical guidelines disagree with Cass.
Myth 1: 98% of all studies in this area were ignored.
Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation.
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
The systematic review on interventions to suppress puberty (Taylor et al: Puberty suppression) provides an update to the NICE review (2020a). It identified 50 studies looking at different aspects of gender-related, psychosocial, physiological and cognitive outcomes of puberty suppression. Quality was assessed on a standardised scale. There was one high quality study, 25 moderate quality studies and 24 low quality studies. The low quality studies were excluded from the synthesis of results.
Independent review of gender identity services for children and young people: Interim report (the “Cass Review”).- https://cass.independent-review.uk/publications/interim-report/
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.
12 cohort, 9 cross-sectional and 32 pre–post studies were included (n=53). One cohort study was high-quality. Other studies were moderate (n=33) and low-quality (n=19). Synthesis of high and moderate-quality studies showed consistent evidence demonstrating induction of puberty, although with varying feminising/masculinising effects. There was limited evidence regarding gender dysphoria, body satisfaction, psychosocial and cognitive outcomes, and fertility.
Taylor J, Mitchell A, Hall R, et al
Masculinising and feminising hormone interventions for adolescents experiencing gender dysphoria or incongruence: a systematic review
Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326670
Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,
One emerging criticism of the Cass review is that it set the methodological bar too high for research to be included in its analysis and discarded too many studies on the basis of quality. In fact, the reality is different: studies in gender medicine fall woefully short in terms of methodological rigour; the methodological bar for gender medicine studies was set too low, generating research findings that are therefore hard to interpret. The methodological quality of research matters because a drug efficacy study in humans with an inappropriate or no control group is a potential breach of research ethics. Offering treatments without an adequate understanding of benefits and harms is unethical. All of this matters even more when the treatments are not trivial; puberty blockers and hormone therapies are major, life altering interventions. Yet this inconclusive and unacceptable evidence base was used to inform influential clinical guidelines, such as those of the World Professional Association for Transgender Health (WPATH), which themselves were cascaded into the development of subsequent guidelines internationally.
BMJ 2024;385:q837
Myth 2: Cass recommended no Trans Healthcare for Under 25s.
Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
Taking account of all the above issues, a follow-through service continuing up to age 25 would remove the need for transition at this vulnerable time and benefit both this younger population and the adult population. This will have the added benefit in the longer-term of also increasing the capacity of adult provision across the country as more gender services are established.
Cass Review 19.28 p224
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”
Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions
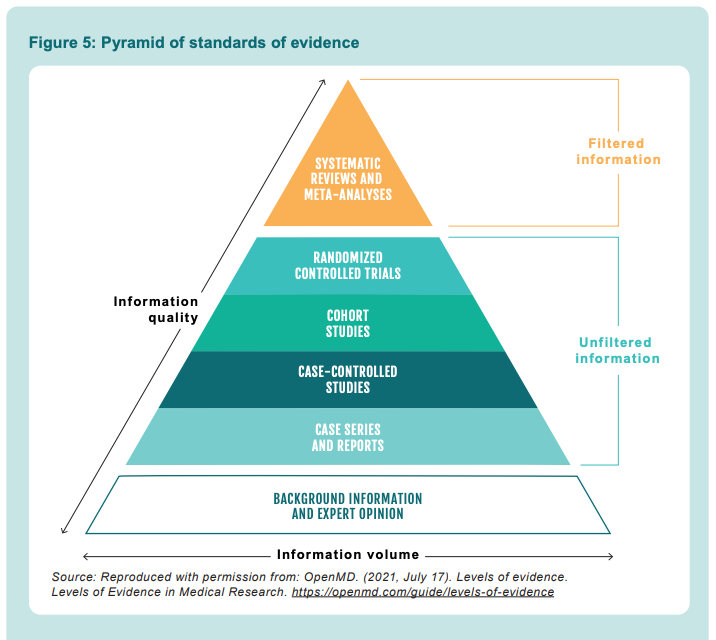
The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1.
Explainer on the Newcastle Ottawa Scale
The Newcastle-Ottawa Scale (NOS) is a tool designed to assess the quality of non-randomized studies, particularly observational studies such as cohort and case-control studies. It provides a structured method for evaluating the risk of bias in these types of studies and has become widely used in systematic reviews and meta-analyses.
The NOS consists of a set of criteria grouped into three main categories: selection of study groups, comparability of groups, and ascertainment of either the exposure or outcome of interest. Each category contains several items, and each item is scored based on predefined criteria. The total score indicates the overall quality of the study, with higher scores indicating lower risk of bias.
This scale is best applied when conducting systematic reviews or meta-analyses that include non-randomized studies. By using the NOS, researchers can objectively assess the quality of each study included in their review, allowing them to weigh the evidence appropriately and draw more reliable conclusions.
One of the strengths of the NOS is its flexibility and simplicity. It provides a standardized framework for evaluating study quality, yet it can be adapted to different study designs and research questions. Additionally, the NOS emphasizes key methodological aspects that are crucial for reducing bias in observational studies, such as appropriate selection of study participants and controlling for confounding factors.
Another advantage of the NOS is its widespread use and acceptance in the research community. Many systematic reviews and meta-analyses rely on the NOS to assess the quality of included studies, making it easier for researchers to compare and interpret findings across different studies.
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
The national infrastructure should be put in place to manage data collection and audit and this should be used to drive continuous quality improvement and research in an active learning environment.
Recommendation 18, The Cass Review. p215
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.
Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:
Estimates of the percentage of individuals who embark on a medical pathway and subsequently have regrets or detransition are hard to determine from GDC clinic data alone.
There are several reasons for this:
- those who do detransition may not choose to return to the gender clinic and are hence lost to follow-up
- the Review has heard from a number of clinicians working in adult gender services that the time to detransition ranges from 5-10 years, so follow-up intervals on studies on medical treatment are too short to capture this
- the inflection point for the increase in presentations to gender services for children and young people was 2014, so even studies with longer follow-up intervals will not capture the outcomes of this more recent cohort.
Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
Gender dysphoria during childhood does not inevitably continue into adulthood. Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children.
World Professional Association for Transgender Health. (2012). Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People [7th Version]. https://www.wpath.org/publications/soc
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
The comments about the quality of evidence are exactly the same as those spouted by homeopaths who claim that if you look at all the evidence, then homeopathy works. By ‘all the evidence’ they include all the badly conducted, highly biased, small-scale trials and pilot studies, customer satisfaction surveys, patient-reported outcomes, return customers, sales of their sugar pills and, of course, Dana Ullman’s personal testimony – if you include of them with no filter for quality, then homeopathy ‘works’ (apparently). Unfortunately, when you set aside all the crappy evidence because it cannot be trusted, homeopathy just doesn’t work.
And you can bet your last penny there will have been much digging into Hilary Cass’s background trying to find some dirt they can use against her to ‘discredit’ her.
Human beings are such arseholes.
There actually are quite a lot of problematic associations with Ron DeSantis
It’s uncannily similar to the reactions of CEASE therapists, GcMAF/MMS touts, etc when confronted by a lack of robust evidence for their autism “cures”.
Thanks for doing this, Andy. I suspect it’s going to be useful to have a single repository that addresses the increasing number of fabrications and myths.
What a horrible thing to say.
Also totally delusional
Grow up Vinnie.
Those cartoons are positively libellous, not that libel actions have a happy history but to set Cass up as a deliberate liar in cartoon format for kids is really scummy behaviour. Who produced them and what sort of distribution are they getting through trans advocacy orgs?
Guillaume “Sophie” Labelle, a man who pretends to be a woman, pedo diaper fetishist and “professional cartoonist”.
No relation to any trans advocacy orgs and no support by them AFAIK- they’re the work of a web cartoonist named Sophie Labelle who distributes them independently via twitter, tumblr, fb, patreon and webtoons via the handle/title Assignedmale. She has a mixed reputation in the online trans community as far as I can tell- a bit of a following but also a reputation for toxicity and preachiness that that some feel are a detriment to their community/generally annoying. Opinions on the art style itself are irrelevant but they’re also not particularly positive. I agree they’re scummy and I would have serious issues with any advocacy org that distributed them and expected to be taken seriously.
(Not to criticize or detract from the content of the post at all but as an artist myself i’d like to encourage Andy to visibly source/cite images he uses when possible, just so readers can look them up without relying on tineye or someone who recognizes the art just happening to stumble upon it. That being said, as someone who’s been trying to take in and form an opinion on the vast amount of information and talk available around this report I really appreciate this breakdown and found it well written and clear- it’s definitely gained him a new reader.)
Blockers saved my life almost a decade ago. It’s sad to see the UK seemingly moving to make it increasingly harder for trans citizens to access them.
It is indeed stunning and brave to put an unevidenced, anecdotal claim on this web site.
The points you’ve made under the Myth 4 subheading suggest a misreading of the report. It says clearly 3,499 patients were audited and 3,306 were included in the analysis, with fewer than ten detransitioning. It is completely unfounded to imply the proportion of detransitioners amongst that 3,306 is actually far higher. You especially should not be doing it under bold headers saying ‘Myth’ and ‘Fact’.
Ironically you’ve also quoted Cass’s mathematical illiteracy. Referrals data doesn’t exhibit an inflexion point in 2014. An inflexion would imply that an accelerating trend became a decelerating one, or vice versa. She clearly doesn’t know what inflexion point means. Of course, ironically, the true inflexion point in the referrals data is later on, where the growth flattens off. This is something Cass repeatedly truncates from graphs and tables to justify scary lines about exponential growth. Perhaps that should appear in your list of myths…
“It says clearly 3,499 patients were audited and 3,306 were included in the analysis, with fewer than ten detransitioning”
And, as mentioned in the Cass Review, we also know that audit has shortcomings due to issues like patients being lost to follow-up. In short, while we know that a few of those 3,306 patients definitely detransitioned, we can’t rule out more of them ended up detransitioning but were not recorded as having done so.
I’ve looked over Appendix 8 to find anything intimating what you are saying, and I’ve found nothing. The language is clear, it explicitly states that fewer than ten patients, from that analysed 3,306 detransitioned back to their natal gender.
It’s quite telling that there is a push to effectively debunk this one part of the Cass review, while glaringly misleading information is tolerated, e.g. “The numbers of children and young people presenting to the UK NHS Gender Identity Service (GIDS) has been increasing year on year since 2009, with an exponential rise in 2014”.
Your first point has been dealt with. It is myth to claim less than 10 kids detransitioned. We simply do not know what the true number is.
Your second point is a quibble. We can all understand the rate of change of referrals changes dramatically around 2014, even if it is not strictly a mathematical inflexion point.
… dealt with indeed.
As for the second point, this is much more serious than a single mathematical term being used incorrectly. Throughout the review Cass makes inaccurate statements about GIDs referrals data, one of which I have quoted above. In two cases those inaccurate statements are illustrated by tables/graphs, but the dataset has been inexplicably truncated. That truncation fundamentally alters the trend’s appearance.
Cass not knowing what an inflexion point is suggests weak mathematical literacy. Cass not knowing what exponential means is deeply problematic. Cass misleading her audience by truncating a dataset is outrageous. Even if we assume that the error was entirely unintentional, it undermines the notion that the review was unbiased and scientifically rigorous.
“The language is clear, it explicitly states that fewer than ten patients, from that analysed 3,306 detransitioned back to their natal gender.”
You’re missing four words from the end of that sentence: “that we know of.” Without those four words, that sentence is misleading at best, dishonest at worst.
You seem ignorant of the implications of what it means for patients to be lost to follow-up. At least I hope that’s the case because the alternative is that you are being dishonest. Either way, you calling someone else mathematically illiterate is very much a case of throwing stones from a glass house. I’m not much for quoting Bible verses, but seriously, get the log out of your own eye!
The sentence I’m quoting, from a key findings table, doesn’t contain the words ‘that we know of’ or anything to that effect. What a weird and specific lie.
Quite remarkable how hard you’re pushing this faith based belief that there are loads of detransitioners hiding somewhere. Cass and her team had four years to find them, clearly wanted to find them, and found fewer than ten. There’s really no way to spin this, however much religious faith you may have in your conspiracy theory: detransition rates and regret rates aren’t high compared to other interventions. There is nothing in Appendix 8 to suggest that there is a mass of detransitioners hiding under a rock, or in another castle.
It’s also telling that neither person responding to me has made any attempt to defend the criticism I’ve levelled at the way she has misleading presented statistics. It’s almost as if it’s inexcusable.
“The sentence I’m quoting, from a key findings table, doesn’t contain the words ‘that we know of’ or anything to that effect.”
What you said after “The language is clear” is a paraphrase, not a quote. The “that we know of” is implied from several of those 3,306 being lost to follow-up.
I’m going to assume (pretend?) that you don’t know what lost to follow-up means. It means that GIDS lost track of many of those 3,306 patients and doesn’t know what happened to them. It’s possible that none of them (besides that original fewer than 10 number) detransitioned, or that 3.14159265% detransistioned, or 27.18281828459045% did, or whatnot. WE DON’T KNOW BECAUSE GIDS LOST TRACK.
It’s not a matter of faith to recognize limitations in the data that make the facts of the matter uncertain. Rather, it’s assuming that no one else detransitioned because no one knows otherwise is the “faith based belief”.
“It’s also telling that neither person responding to me has made any attempt to defend the criticism I’ve levelled at the way she has misleading presented statistics.”
Gee, maybe it’s your “criticism” amounts to unsupported bold claims. There’s no “there” there.
And another thing: “Cass and her team had four years to find them, clearly wanted to find them, …”
This totally misleads what the review was about. It wasn’t about finding detransitioners, but rather about finding the evidence base for trans healthcare for children, such as it is. Cass isn’t some culture warrior in the TERF wars, however much you’d like her to be.
‘What you said after “The language is clear” is a paraphrase, not a quote. The “that we know of” is implied from several of those 3,306 being lost to follow-up.
I’m going to assume (pretend?) that you don’t know what lost to follow-up means. It means that GIDS lost track of many of those 3,306 patients and doesn’t know what happened to them. It’s possible that none of them (besides that original fewer than 10 number) detransitioned, or that 3.14159265% detransistioned, or 27.18281828459045% did, or whatnot. WE DON’T KNOW BECAUSE GIDS LOST TRACK.
It’s not a matter of faith to recognize limitations in the data that make the facts of the matter uncertain. Rather, it’s assuming that no one else detransitioned because no one knows otherwise is the “faith based belief”.’
The blog you are defending states that ‘The low recorded rates must be due in part to insufficient data availability.’ Not could be. Must be. That one word is actually why I decided to respond to this blog in the first place, it’s the clear tell that someone is working backwards from a conclusion to a justification.
Appendix 8 doesn’t suggest that any of the 3,306 were lost to follow-up. The word lost doesn’t appear, the term follow-up doesn’t appear. At discharge, fewer than ten had detransitioned. Will some detransition later? Sure. Some may also retransition.
The basic question here is… is this actually a myth? Is it a myth that the review found <10 detransitioners out of ~3.5k patients? No. It's literally what was found.
— Gee, maybe it’s your “criticism” amounts to unsupported bold claims. There’s no “there” there.
The Summary and Recommendations is the part of the review designed to be read by the widest audience. On Page 24, Cass has published a statement that is factually inaccurate, and that statement is backed up by a graph that has been inexplicably cut short removing several years worth of data that entirely undermines the statement she has made.
The falsehood that referrals were rising exponentially was spread throughout the media on the day the report was published. Trans people spreading exponentially is a myth, and a dangerous one that suggests viral spread. Cass is responsible for giving that myth booster rockets.
There's nothing bold about my claims.
“Appendix 8 doesn’t suggest that any of the 3,306 were lost to follow-up.”
There’s a slight of hand here. You refer narrowly to Appendix 8 when it’s clear from other parts of the report that loss to follow-up is a problem. From the summary and conclusions:
“87. The percentage of people treated with
hormones who subsequently detransition
remains unknown due to the lack of long-term
follow-up studies, although there is suggestion
that numbers are increasing.”
The obvious conclusion from this is Cass understands that the data in Appendix 8 doesn’t include any long-term follow-up.
“On Page 24, Cass has published a statement that is factually inaccurate, and that statement is backed up by a graph that has been inexplicably cut short”
Cut short? The graph is from the paper “Sex Ratio in Children and Adolescents Referred to the Gender Identity Development Service in the UK (2009–2016)”, and its data runs from 2009 to 2016, the time interval discussed in the paper. You write as if Cass took a graph from the paper and cut off part of it, which didn’t happen.
“There’s nothing bold about my claims.”
You (1) make sweeping claims of mathematical illiteracy that are justified by nits at best, and (2) make claims that the data included in an appendix of a report is complete and lacks any losses to follow-up despite the person including it the report says otherwise. Yes, such claims are bold.
‘Cut short? The graph is from the paper “Sex Ratio in Children and Adolescents Referred to the Gender Identity Development Service in the UK (2009–2016)”, and its data runs from 2009 to 2016, the time interval discussed in the paper. You write as if Cass took a graph from the paper and cut off part of it, which didn’t happen.’
This is remarkable pedantry.
The statement at the top of the page is false. It is contradicted by readily available data. Instead of publishing the available data, she chooses to publish a subset of it that aligns* with the statement. I cannot begin to express how shoddy this is for scientific work.
*roughly aligns. Frankly given Cass’ use of the word exponential throughout the review, she very much falls on the left side of the divide this comic mocks: https://twitter.com/vb_jens/status/1372251931444350976
I love it — you sir are an eloquent parser! I myself am great at confusing the f*ck out of these sad little liberal castrators – Keep up the good fight!!!
Would you like to join our pod? LMK
The White Paper by a team at Yale Law is the most serious and quite damning response to the Cass Review, despite the myths that started circulating about it.
If anyone wants to read an actual peer-reviewed critique of the nonsense in the “Yale Law” paper, do read this.
https://adc.bmj.com/content/early/2024/10/15/archdischild-2024-327994
Extending Andy L’s comment, Jesse Singal has done a very good 3 part takedown of the Yale Law Paper. You should read it, its quite the shitshow that happened over at Yale:
https://jessesingal.substack.com/p/yales-integrity-project-is-spreading
https://jessesingal.substack.com/p/yales-integrity-project-is-spreading-ba7
https://jessesingal.substack.com/p/yales-integrity-project-is-spreading-dbb
Also since the 2024 study cited by Andy L, there has been another study that exposes the falsehoods the Yale report uses:
https://www.tandfonline.com/doi/full/10.1080/0092623X.2025.2455133#abstract